TURBT (Transurethral Resection of Bladder Tumor) is typically needed when a person is suspected to have or has been diagnosed with a bladder tumor, especially at early stages. It plays a crucial role in both diagnosis and initial treatment.
We need TURBT (Transurethral Resection of Bladder Tumor) in the following situations:
1. Diagnosis of Bladder Cancer
When a person has symptoms like:
Blood in urine (hematuria)
Frequent or painful urination
Imaging or cystoscopy shows a suspicious mass or lesion in the bladder.
TURBT helps confirm if the tumor is cancerous, and determines the type, grade, and depth of invasion.
2. Initial Treatment of Early-Stage Bladder Cancer
Especially for non-muscle invasive bladder cancer (NMIBC):
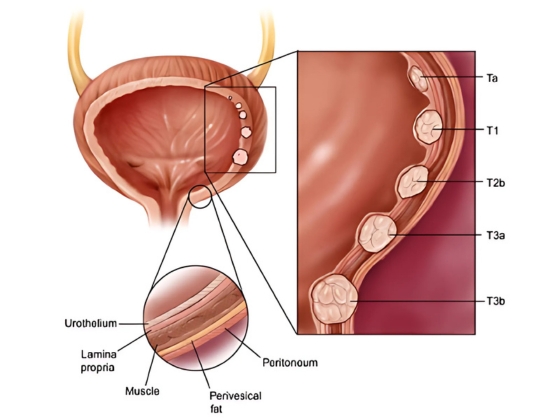
Ta (confined to bladder lining)
T1 (into connective tissue)
CIS (flat carcinoma in situ)
TURBT removes the tumor completely, often followed by intravesical therapy (e.g. BCG).
3. Restaging or Repeat TURBT
If the initial tumor is:
High-grade
T1 stage
A second TURBT (within 2–6 weeks) is often done to ensure complete removal and accurate staging.
4. Relief of Urinary Symptoms in Advanced Cancer
When the tumor causes:
Bleeding
Blockage of urine flow
TURBT may be done for palliative purposes, not cure.
Procedure of TURBT (Transurethral Resection of Bladder Tumor)
1. Preoperative Preparation
Admission: Usually done as a day-care or short hospital stay.
Anesthesia: Spinal or general anesthesia is administered.
Positioning: Patient lies on their back with legs supported in stirrups (lithotomy position).
2. Insertion of the Resectoscope
A resectoscope (a thin tube with a camera and surgical loop) is gently inserted through the urethra into the bladder.
No external incision is made.
3. Visual Inspection of the Bladder
The surgeon examines the inside of the bladder for:
Tumor(s) — their size, location, and number
Bladder wall condition
Any suspicious areas for biopsy
4. Tumor Resection
The tumor is shaved off in layers using the resectoscope’s electric loop.
If necessary, tissue from the base of the tumor (including muscle layer) is also taken to check how deep the tumor has grown.
5. Control of Bleeding (Hemostasis)
The surgical area is cauterized to stop bleeding.
Irrigation fluid is used to flush out blood clots and tissue pieces from the bladder.
6. Tissue Collection for Biopsy
Tumor and bladder wall tissue samples are collected and sent for pathological analysis to determine:
Cancer presence
Type, grade, and stage
7. Catheter Placement
A Foley catheter is inserted into the bladder to:
Drain urine
Prevent blockage from clots
Allow bladder to heal
Bladder irrigation may be used to prevent clot formation.
Postoperative Care
Hospital Stay: Usually 1–2 days depending on recovery.
Catheter Removal: Within 24–72 hours typically.
Pathology Report: Usually ready within 7–10 days to guide further treatment.
Duration of Procedure
Typically takes 30–90 minutes depending on the number and size of tumors.