Introduction
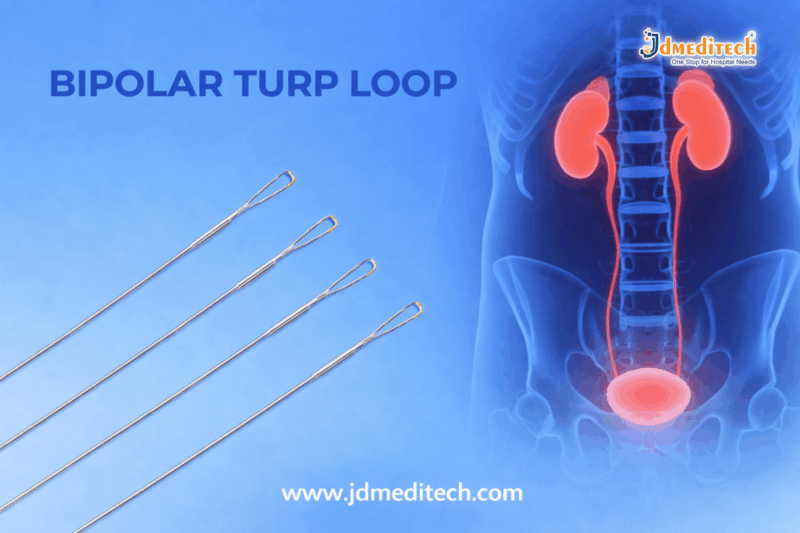
The Precision Monopolar Loop Electrode for Prostate Surgery is a vital component in modern urological procedures, especially in Transurethral Resection of the Prostate (TURP). Designed for high precision and controlled tissue removal, this electrode plays a crucial role in ensuring safe and effective prostate surgery.
With advancements in surgical technology, the demand for reliable and high-performance monopolar loop electrodes has significantly increased. These instruments provide surgeons with excellent cutting efficiency and coagulation control, improving overall patient outcomes.
What is a Precision Monopolar Loop Electrode?
A Precision Monopolar Loop Electrode for Prostate Surgery is a specialized electrosurgical device used in TURP procedures. It is connected to an electrosurgical unit and is designed to cut and coagulate prostate tissue using high-frequency electrical current.
The loop-shaped design allows surgeons to precisely remove obstructive prostate tissue while maintaining visibility and control throughout the procedure.
Key Features of Precision Monopolar Loop Electrode for Prostate Surgery
1. High Precision Cutting
The electrode ensures smooth and accurate tissue resection, minimizing damage to surrounding structures.
2.High Electrical Conductivity
Manufactured with medical-grade materials, it provides efficient energy transmission for consistent performance.
3. Superior Hemostasis Control
It allows effective coagulation, reducing intraoperative bleeding and enhancing surgical safety.
4. Durable Medical-Grade Construction
Built using high-quality stainless steel or tungsten wire loops for long-lasting performance.
5. Compatibility with Standard Resectoscopes
The Precision Monopolar Loop Electrode for Prostate Surgery is designed to work seamlessly with most monopolar TURP systems.
Applications in Prostate Surgery
The Precision Monopolar Loop Electrode for Prostate Surgery is primarily used in:
- Transurethral Resection of the Prostate (TURP)
- Treatment of Benign Prostatic Hyperplasia (BPH)
- Removal of obstructive prostate tissue
- Electrosurgical cutting and coagulation procedures
Advantages of Using Precision Monopolar Loop Electrode
1. Enhanced Surgical Accuracy
Surgeons can perform precise resections with better control, reducing complications.
2. Improved Patient Safety
Efficient coagulation minimizes blood loss and lowers the risk of post-operative complications.
3. Cost-Effective Solution
Compared to advanced technologies, monopolar systems are widely available and economical.
4. Proven Clinical Performance
Monopolar TURP remains a gold-standard procedure in urology, supported by decades of successful outcomes.
How It Works
The Precision Monopolar Loop Electrode for Prostate Surgery works by delivering high-frequency electrical current through the loop. When the loop comes into contact with tissue:
- The current generates heat
- Tissue is cut or vaporized
- Simultaneous coagulation occurs to control bleeding
A grounding pad is used to safely return the electrical current, completing the circuit.
Monopolar vs Bipolar Loop Electrode
| Feature | Monopolar Loop Electrode | Bipolar Loop Electrode |
| Energy Flow | Through body to grounding pad | Localized between electrodes |
| Irrigation Fluid | Non-conductive (glycine) | Saline |
| Cost | More affordable | Higher |
| Usage | Widely used in TURP | Increasingly popular |
Safety Considerations
When using a Precision Monopolar Loop Electrode for Prostate Surgery, it is important to:
- Ensure proper grounding pad placement
- Use compatible electrosurgical units
- Monitor irrigation fluids carefully
- Follow sterilization protocols
- Avoid excessive thermal exposure
Choosing the Right Monopolar Loop Electrode
Selecting the right Precision Monopolar Loop Electrode for Prostate Surgery depends on:
- Loop size and shape
- Material quality
- Compatibility with resectoscope
- Surgeon preference
- Procedure requirements
High-quality electrodes ensure consistent performance and reduce procedural risks.
Maintenance and Handling
Proper care of the Precision Monopolar Loop Electrode for Prostate Surgery enhances its lifespan:
- Clean and sterilize after each use
- Inspect for damage or wear
- Store in sterile conditions
- Follow manufacturer guidelines
Conclusion
The Precision Monopolar Loop Electrode for Prostate Surgery remains an essential tool in TURP procedures. Its ability to deliver precise cutting and effective coagulation makes it a trusted choice among urologists worldwide.
With its proven efficiency, cost-effectiveness, and reliability, this device continues to play a critical role in improving prostate surgery outcomes.
Get Connected:
+91 79909 93062 | +91 63513 72032 | exports@jdmeditech.com